Ultrasound - Focused 1st Trimester Pregnancy, Transvaginal Exam
Ultrasound: Focused 1st Trimester Pregnancy (Transvaginal Assesment)
Goals:
- Confirm intrauterine pregnancy (IUP) and estimating its viability
- Look for signs of ectopic pregnancy
Transducer: High-frequency endocavitary transducer
Windows: Transvaginal view using cervix as window
1. Coronal / transverse view
Directional indicator: Pointed to patient’s right side

Figure 1: Appropriate transducer orientation for the coronal transvaginal exam

Figure 2: Ectopic pregnancy on transvaginal ultrasound, coronal view. Shown is a yolk sac within an extra-uterine gestational sac (black arrow) adjacent to an empty endometrium (e), outside of the uterus.
2. Sagittal / longitudinal view
Directional indicator: Pointed to anterior of patient (towards the ceiling)

Figure 3: Appropriate transducer orientation for the sagittal transvaginal exam
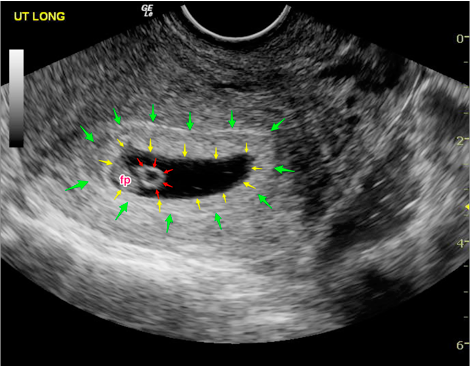
Figure 4: Intrauterine pregnancy on transvaginal ultrasound, sagittal view. Shown is a gestational sac containing a yolk sac and within the endometrium.
Both of these windows include a complete sweep through the uterus in each direction looking for a gestational sac and yolk sac or fetal pole within the endometrium.
Interpretation and Tips
An IUP for point-of-care purposes is defined as a yolk sac or fetal pole within a gestational sac within the endometrium. This indirectly excludes an ectopic pregnancy in an appropriate clinical setting.
Consider measuring the distance between the gestational sac and the edge of uterus. If this endomyometrial mantle thickness is <8 mm, then consider the possibility of an interstitial ectopic pregnancy.
An ectopic pregnancy will occasionally be seen as an extrauterine mass. However, free fluid in a pregnant patient without an IUP should also be considered an ectopic pregnancy until proven otherwise.
Pitfalls
Inserting the transducer too deeply.
- The transducer should be inserted to the cervix, using it as a window. If you continue to push once at the cervix, the transducer will frequently slide into the posterior fornix and only bowel/rectum will be seen.
Scanning with a full bladder.
- While the transabdominal approach is enhanced by a full bladder, the patient should empty their bladder prior to transvaginal scanning to improve visualization.
Calling a gestational sac an IUP.
- At least a yolk sac is needed. A pseudogestational sac with an ectopic pregnancy is possible.
Relying on the quantitative beta-HCG and “discriminatory zone” for decision-making.
- Over 40% of ectopic pregnancies will have beta-HCG levels below the discriminatory zone.
Considering an “inconclusive scan” negative for ectopic.
- Ectopic pregnancies are almost always ruled-out by finding an IUP. Absence of an extrauterine mass does not exclude ectopic pregnancy.
Failure to recognize specific high-risk populations.
- Patients undergoing assisted reproductive therapy have a much higher (1-3%) incidence of heterotopic pregnancy. Identification of an IUP does not exclude a co-existing ectopic in this group.
References
- Wang R, Reynolds TA, West HH, et al. Use of a β-hCG discriminatory zone with bedside pelvic ultrasonography. Ann Emerg Med. 2011;58(1):12-20. [PubMed]
- Tayal VS, Cohen H, Norton HJ. Outcome of patients with an indeterminate emergency department first-trimester pelvic ultrasound to rule out ectopic pregnancy. Acad Emerg Med. 2004;11(9):912-7. [PubMed]
