Toxic Alcohol Ingestion - Methanol
Toxic Alcohol Ingestion: Methanol
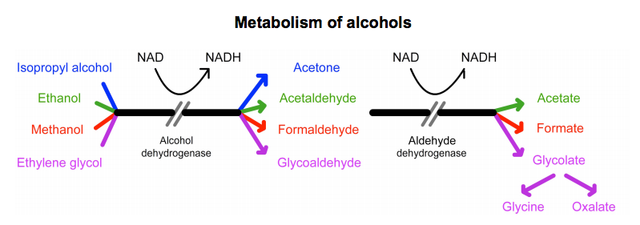
General concepts for all 3 toxic alcohols:
- Parent compounds (not metabolites) cause high osmolal gap
- When NAD depleted, pyruvate converts to lactate - which then causes lactic acidosis
- See metabolism of alcohols diagram below
Methanol: Factoids
Solvent found in cleaning and printing solutions, adhesives, stains, paint removers, antifreeze agent in windshield wiping fluid, camp stove fuel, gasoline additive
Pharmacology:
- Peak serum concentration 30-60 minutes, elimination half-life 12-20 hours
- Permanent blindness reported at as little as 0.1 mL/kg (6-10 mL in adults)
- Lethal dose = 1-2 mL/kg
- Metabolite (eg. formic acid) causes toxicity, but does NOT cause osmolal gap
Classic Presentation
Classic Profile
- Altered mental status
- Visual disturbances
- Abdominal pain
- High anion gap metabolic acidosis
- High osmolal gap
Signs and Symptoms
- CNS: Headache, lethargy, confusion, Parkinsonian extrapyramidal symptoms
- Ocular: Blurry vision, central scotoma, impaired pupillary response, photophobia, retinal edema (permanent damage in 25-33% of patients)
- GI: Vomiting, abdominal pain, pancreatitis
Stages of Presentation
| Stage | Clinical findings |
|---|---|
| Early | Mild euphoria, inebriation, drowsiness |
| Latent (lasting 6-30 hours) | Normal sensorium but blurred vision |
| Late | Severe systemic toxicity with worsening acidosis |
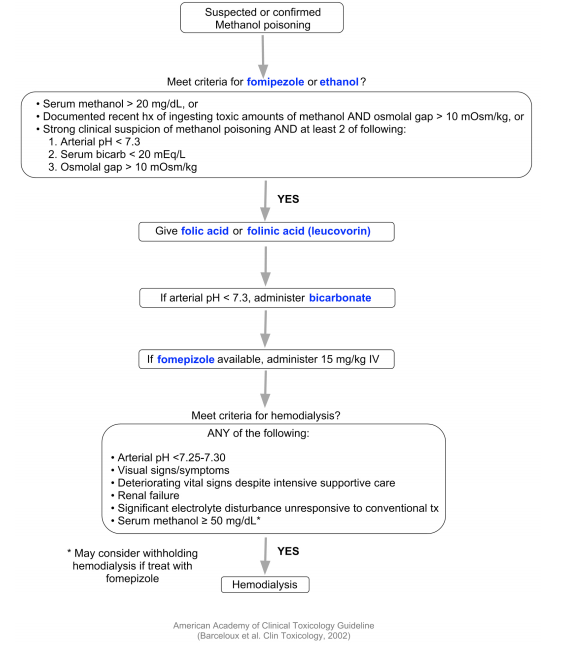
Management
Goal: Prevent further formation of formic acid (using fomepizole) and eliminate toxic metabolites (through dialysis)
- Folic or folinic acid supplementation to enhance formate metabolism
- Antidote: Fomipezole inhibits alcohol dehydrogenase (alternative = ethanol)
| Fomipezole | Dosing |
|---|---|
| Loading dose | 15 mg/kg IV |
| Maintenance dose | 10 mg/kg IV every 12 hours x 2 days |
American Academy of Clinical Toxicology guidelines
Metabolism of alcohols
References
- Jammalamadaka D, Raissi S. Ethylene glycol, methanol and isopropyl alcohol intoxication. Am J Med Sci. 2010 Mar;339(3):276-81. doi: 10.1097/MAJ.0b013e3181c94601. [PubMed]
- Kraut JA, Kurtz I. Toxic alcohol ingestions: clinical features, diagnosis, and management. Clin J Am Soc Nephrol. 2008 Jan;3(1):208-25. Epub 2007 Nov 28. [PubMed]
- Marraffa JM, Cohen V, Howland MA. Antidotes for toxicological emergencies: a practical review. Am J Health Syst Pharm. 2012 Feb 1;69(3):199-212. doi: 10.2146/ajhp110014 [PubMed]
- Barceloux DG, Bond GR, Krenzelok EP, Cooper H, Vale JA; American Academy of Clinical Toxicology Ad Hoc Committee on the Treatment Guidelines for Methanol Poisoning. American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning. J Toxicol Clin Toxicol. 2002;40(4):415-46. [PubMed]
