Ultrasound DVT Assessment
Ultrasound: Focused Deep Venous Thrombosis (DVT) Assessment
*Goals: *Evaluate for DVT using the 2-point compression technique, focusing on the highest probability areas: femoral and popliteal veins
*Transducer: *High frequency linear transducer. Directional indicator to patient’s right in transverse position
*Pt position: *Externally rotated hip, flexed knee, +/- reverse Trendelenburg
1. Femoral Vein
- Place linear transducer in transverse position at level of inguinal ligament
- Identify the confluence of femoral vein and greater saphenous vein (saphenofemoral junction [SFJ]), and apply direct pressure to assess for compressibility
- To fully evaluate the common femoral vein, slide 5 cm distal to the confluence, compressing at 0.5-1 cm intervals. This allows for visualization of the proximal portion of the deep and superficial femoral veins. Assess for compressibility in both.
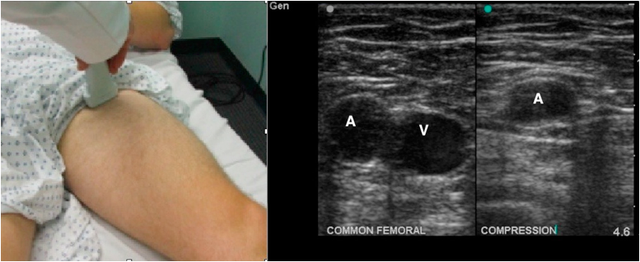
Figure 1: Transducer location to evaluate the femoral vein and normal ultrasound images showing common femoral artery (A) and fully compressible vein (V).
2. Popliteal Vein
- Place linear transducer in transverse position in popliteal fossa.
- Locate the popliteal artery and vein, and assess for compressibility of vein.
- To fully evaluate the popliteal region, slide distally following the popliteal vein to allow for visualization of the proximal portion of the anterior and posterior tibial veins, and the peroneal vein. At this trifurcation, assess for compressibility of all three veins.
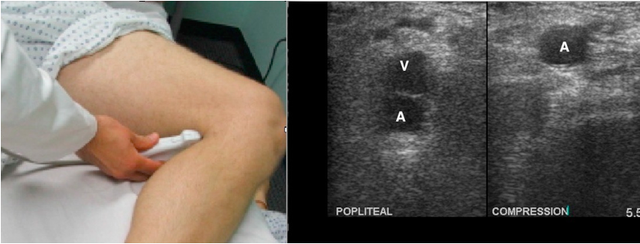
Figure 2: Transducer location to evaluate the popliteal vein and normal ultrasound images showing popliteal artery (A) and fully compressible vein (V).
Positive (Abnormal) DVT Study
A non-compressible vein indicates a positive study for thrombosis.
Normally, there should be complete coaptation of the venous walls – a.k.a. the walls collapse against one another. If the vein does not full compress, one assumes there is an intraluminal thrombus.
Note: While the thrombus is frequently visualized as a discrete echogenic structure, it may not always be seen.
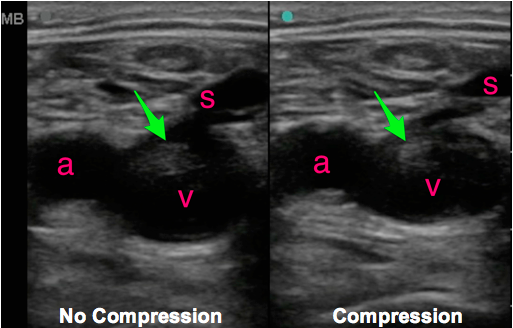
Figure 3: Positive DVT study showing thrombus in the femoral vein (v), adjacent to the femoral artery (a) and involving the greater saphenous vein (s). The image on the right demonstrates that the vein does not collapse with compression.
Struggling with the Exam?
Larger or edematous patients? Use the curvilinear probe if you can’t visualize the deep veins.
Can’t compress vein, but can’t visualize clot? Assume that there is a DVT, as clots can be isoechoic with the surrounding blood and may not be directly visualized. Direct visualization of the thrombus is not required for a positive study.
Difficulty finding the popliteal vein? The popliteal vein can be difficult to identify. Try having the patient hang the legs over the edge of the bed to distend the vessels or position the patient in the prone position while passively flexing the knee with the foot in the air. Color Doppler may also help identify the vessels.
Not sure if the vein is fully compressing? A normal vein will completely disappear when compressed. Make sure to center the vein on the screen and apply pressure evenly. If pressure is not applied directly perpendicular to the skin, the vessel may appear not to collapse due to unevenly distributed pressure.
How much pressure is enough? An appropriate amount of pressure gives complete collapse of the vein as well as some (but not full) compression of the adjacent artery.
Common Errors
- Other structures, such as lymph nodes, may mimic a thrombus. Be sure to scan through the entire structure as a lymph node will appear discrete and separate from the vessels.
- To fully evaluate the common femoral vein, make sure to visualize the proximal region at the confluence of the greater saphenous and common femoral veins.
References
Kline JA, O'malley PM, Tayal VS, Snead GR, Mitchell AM. Emergency clinician-performed compression ultrasonography for deep venous thrombosis of the lower extremity. Ann Emerg Med. 2008;52(4):437-45.[[PubMed]((www.ncbi.nlm.nih.gov/pubmed/18562044)]
Bernardi E, Camporese G, Büller HR, et al. Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deep vein thrombosis: a randomized controlled trial. JAMA. 2008;300(14):1653-9.[PubMed]
