Ketofol
Ketamine and Propofol (Ketofol) for Procedural Sedation
Take Home Points
- Ketofol is a combination of ketamine and propofol.
- Ketamine gives you a dissociative sedative, analgesic, and amnestic effect.
- Propofol gives you rapid sedation and antiemetic effects.
- Overall, it appears that ketofol could have a slightly better time to sedation, and length of sedation, but this is not statistically significant based on available evidence. However, it does appear that ketofol does have a more steady sedation depth not requiring as many subsequent doses.
- More studies needed (it would be great to see a three-armed study comparing ketofol, ketamine, and propofol with appropriate and clinically equivalent dosing for each).
Ketamine Basics

Ketamine is a dissociative anesthetic that is a phencyclidine derivative and provides sedation, analgesia, and amnesia. It works by inhibiting catecholamine uptake, which exerts a sympathomimetic effect.
Typical dose: 1–2 mg/kg IV or 4–5 mg/kg IM
- Additional doses may be required at increments of 0.5-1 mg/kg.
Major adverse outcomes: airway obstruction, hypoxia, apnea, and laryngospasm.
- In a meta-analysis, of 8,282 patients, Green et al (2009) stated that the total incidence of these major adverse outcomes was only 3.9%.
- Vomiting occurs in about 7–26% of patients.
What about the elevated intraocular pressure (IOP) and intracranial pressure (ICP) that we are always hearing about?
Drayna et al (2011) found minimal, transient elevations of IOP that were not clinically meaningful.
- The largest difference from baseline IOP occurred at 15 minutes with an estimated change of only 1.09 mmHg.
Propofol Basics
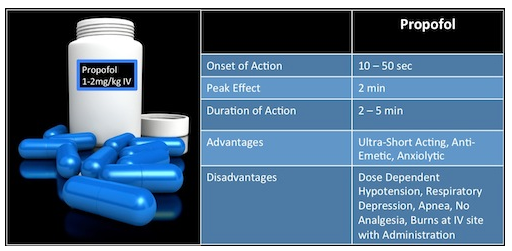
Propofol is a lipophilic, ultra short-acting hypnotic agent, which works by potentiating GABA receptors on the neuronal lipid membranes. It does not provide any analgesia, and therefore should not be used as a sole agent for sedation. Note that one of its advantages is its anti-emetic property with a very low incidence of vomiting.
Typical dosing: 1-2 mg/kg bolus followed by either a continuous infusion at 0.05-0.1 mg/kg/min or by 0.5 mg/kg boluses every 2–3 minutes. The Pediatric Sedation Research Consortium looked at 49,836 propofol sedation cases and found no instances of death associated with propofol.
- CPR was required in 2 cases, aspiration occurred in 4 cases, oxygen desaturation (less than 90% for longer than 30 sec duration) occurred in 716 cases, and central apnea occurred in 143 cases.
HOW DO YOU MIX KETOFOL?
No standard dosing regimen established.
Most studies and authors recommend a 1:1 ratio to provide ease of administration. The medications can be mixed or given sequentially.
Click here for full ALiEM blog post
References
- Drayna PC, Estrada C, Wang W, Saville BR, Arnold DH. Ketamine sedation is not associated with clinically meaningful elevation of intraocular pressure. Am J Emerg Med. 2012 Sep;30(7):1215-8. [PubMed]
- Cravero JP, Beach ML, Blike GT, Gallagher SM, Hertzog JH; Pediatric Sedation Research Consortium.. The incidence and nature of adverse events during pediatric sedation/anesthesia with propofol for procedures outside the operating room: a report from the Pediatric Sedation Research Consortium. Anesth Analg. 2009 Mar;108(3):795-804. [PubMed]
- Alletag MJ, Auerbach MA, Baum CR. Ketamine, propofol, and ketofol use for pediatric sedation. Pediatr Emerg Care. 2012 Dec;28(12):1391-5; quiz 1396-8. [PubMed]
- Shah A, Mosdossy G, McLeod S, Lehnhardt K, Peddle M, Rieder M. A blinded, randomized controlled trial to evaluate ketamine/propofol versus ketamine alone for procedural sedation in children. Ann Emerg Med. 2011 May;57(5):425-33.e2. [PubMed]
- Andolfatto G, Abu-Laban RB, Zed PJ, Staniforth SM, Stackhouse S, Moadebi S, Willman E. Ketamine-propofol combination (ketofol) versus propofol alone for emergency department procedural sedation and analgesia: a randomized double-blind trial. Ann Emerg Med. 2012 Jun;59(6):504-12.e1-2. [PubMed]
- Green SM, Roback MG, Krauss B, Brown L, McGlone RG, Agrawal D, McKee M, Weiss M, Pitetti RD, Hostetler MA, Wathen JE, Treston G, Garcia Pena BM, Gerber AC, Losek JD; Emergency Department Ketamine Meta-Analysis Study Group. Predictors of airway and respiratory adverse events with ketamine sedation in the emergency department: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med. 2009 Aug;54(2):158-68.e1-4.[PubMed]
