Knee Examination
Knee Examination
Solomon et al, JAMA 2001
- Meta-analysis study: The accuracy of the clinical knee exam in detecting meniscal or ligamentous injury
Anatomy of the Knee Joint
- Largest articulation in body
- Stabilized by ACL, PCL, MCL, LCL, menisci, capsule and muscle
- ACL and PCL also aid in proprioception
- Medial meniscus: Because it more immobile than the lateral meniscus, it is more commonly injured.
Anterior Cruciate Ligament (ACL) Injury
Mechanism: Knee twist with tibia pushed anteriorlyusually with concurrent valgus stress
Symptoms
- May recall “pop” sound at injury
- May c/o knee buckling or “giving out”
- May notice more pronounced pain when pivoting
Exam
- Lachman test
- Anterior drawer sign
- Lateral pivot shift test: Valgus stress on knee plus internal/external rotation of knee during knee flexion
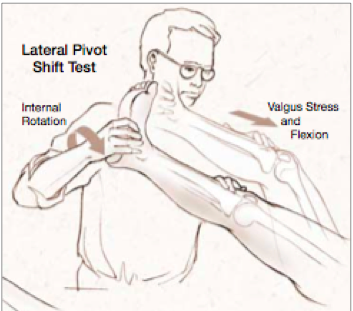
Pivot Shift YouTube video
Posterior Cruciate Ligament (PCL) Injury
- Knee twist with tibia pushed posteriorly
- Composite stats for posterior drawer sign:
- Positive LR 21
- Negative LR 0.05
Meniscus Tear
- Menisci have no pain fibers and pain comesfrom traction on peripheral structures
- 16% asymptomatic patients have meniscustear on MRI (36% if age>45)
- Medial meniscus tear can result in knee locked in flexion (unlikely lateral meniscus because more mobile)
- Association with “clicking” noise when walking
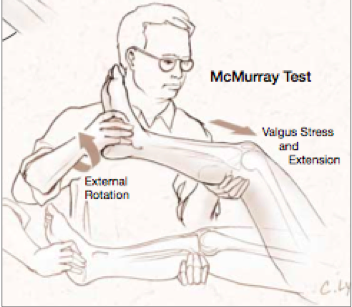
- Exam: McMurray test - British Journal of Sports Med YouTube video
- Lateral meniscus test: Valgus stress on knee and internal/external rotation while flex/extending knee
- Medial meniscus test: Varus stress on knee and internal/external rotation while flex/extending knee
- Exam: Apley compression test - British Journal of Sports Med YouTube video
- In a patient prone position, flex knee to 90 degrees and external/internal rotate knee while axially loading
- Exam: Medial-lateral grind test: Valgus and varus stress on knee while flex/extending knee – other hand is placed at joint line to detect grinding
- Composite stats on exam maneuvers:
- Positive LR 2.7, Negative LR 0.4 (Overall - not that great)
Knee Exam
Conduct exam first on normal knee for comparison
Inspection: Look for atrophy, effusion
- Tip: Collateral ligament injuries often have no effusion in acute setting
Palpation: Look for crepitus as sign of cartilage disruption, joint line tenderness
Function: Perform stress maneuvers
Check for Historical Clues
- Typical effusion onset: Immediate = meniscus or cruciate ligament tear
- Pop noise at time of injury = ACL tear
- Clicking/locking sensation = Meniscus injury
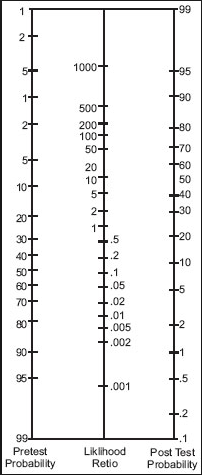
Fagan Nomogram
References
- Solomon DH et. al.The rational clinical examination. Does this patient have a torn meniscus or ligament of the knee? Value of the physical examination. JAMA. 2001 Oct 3;286(13):1610-20. [PubMed]
